Deine Spende

Voraussetzungen für Deine Spende
Eine Spende bedeutet für viele Patienten die letzte Chance auf Leben. Der Erfolg der Blutstammzellspende hängt dabei stark vom Gesundheitszustand des Patienten ab. Die Heilungschancen liegen durchschnittlich bei 40 bis 70%.
Vor diesem Hintergrund behandeln wir jede einzelne Spende mit größter Wertschätzung und all unserer langjährigen Erfahrung. Bei uns ist nicht nur Deine Spende gut aufgehoben, sondern auch Du selbst. Dein Wohlergehen steht im Vordergrund unserer täglichen Arbeit!
Vor Deiner Spende klärt Cellex, ob Du spendefähig bist. Das bedeutet, es wird im Rahmen der Voruntersuchung festgestellt, ob Du gesundheitlich in der Lage bist, zu spenden. Nur wenn für Dich und auch für den Empfänger Deiner Spende keine gesundheitlichen Risiken durch die Spende bestehen, kommst Du für uns als Spender in Frage.
Für Fragen jeglicher Art vor und nach der Spende steht Dir unser medizinisches Team rund um die Uhr zur Verfügung (+49 162 7162560).
So einfach ist eine Blutstammzellspende
Arten von Spenden
Es gibt zwei verschiedene Arten von Spenden – die Blutstammzellspende, bei der die Zellen mittels Apherese entnommen werden, und die Knochenmarkspende.
Grundsätzlich kannst Du Dich für eine der beiden Entnahmearten entscheiden, und wir versuchen natürlich, Deinen Wunsch nach einer bevorzugten Entnahmeart zu erfüllen. Es kann allerdings sein, dass Du als Spender nur für eine der Entnahmemethoden in Frage kommst. Welche Methode aus medizinischen Gründen bevorzugt oder sogar notwendig ist hängt von der Situation des Empfängers ab. Prinzipiell wäre es optimal, wenn Du zu beiden Entnahmearten bereit bist.
Beim Großteil der Spenden erfolgt die Entnahme der Stammzellen mittels einer so genannten „peripheren Stammzellentnahme”. Und das ist ganz einfach!
Deine Stammzellen befinden sich im Knochenmark. Damit sie entnommen werden können, müssen die Stammzellen im Vorfeld der Spende ins Blut ausgeschwemmt werden. Dafür musst Du dir in den fünf Tagen vor der Zellentnahme das hormonähnliche Präparat (G-CSF) unter die Haut spritzen oder von einer medizinischen Fachkraft spritzen lassen.
Unter G-CSF versteht man den Granulozyten-Kolonien stimulierenden Faktor. Bei dem Präparat handelt es sich um ein Zytokin, also einen Botenstoff, der auch natürlich im Körper vorkommt und die Blutbildung in Deinem Körper beeinflusst. Es wird immer dann aktiv, wenn der Körper eine Infektion hat und die „Abwehrzellen“ mobilisiert werden müssen. Das Spritzen des Präparates bewirkt, dass die im Knochenmark vorkommenden Stammzellen in den Blutkreislauf gelangen.
Die ausgeschwemmten und später entnommenen Stammzellen bilden sich innerhalb weniger Wochen nach.
Während der Mobilisierung der Stammzellen können als mögliche Nebenwirkungen grippeähnliche Symptome auftreten, vor allem Knochen- und Gliederschmerzen. Diese können mit einem leichten Schmerzmittel wie Paracetamol behandelt werden.
Nach Deinem Eintreffen im Collection Center erfolgt ein kurzer Gesundheitscheck. Deine Spende wird dann mit Hilfe einer Apheresemaschine durchgeführt, die das Blut durch Zentrifugalkraft in die einzelnen Bestandteile auftrennt und so das Sammeln der entsprechenden Zellen aus dem Blut ermöglicht. Dafür wird Dir an beiden Armen ein venöser Zugang gelegt, der über ein steriles Einmal-System mit der Apheresemaschine verbunden ist.
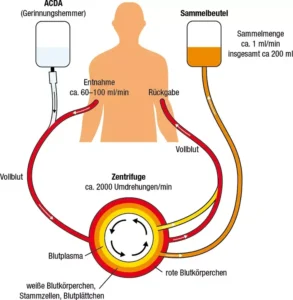
Dein Blut verlässt den Körper auf der einen Seite, fließt durch die Maschine und wird auf der anderen Seite über den zweiten Zugang wieder in den Körper zurückgeführt.
Während des Vorgangs wird ein kleiner Teil deines Blutes, und zwar die für den Patienten wichtigen Stammzellen, absorbiert. Um Blutgerinnungen zu vermeiden, wird dabei ein Gerinnungshemmer eingesetzt, der Zitronensäure ähnelt und vom Körper sehr schnell abgebaut wird. Dadurch kann allerdings kurzzeitig Kribbeln im Mund- und Lippenbereich oder beispielsweise in den Fingern verursacht werden. Durch Kalziumgaben können diese Beschwerden aber rasch beseitigt werden.
Hier findest Du alle relevanten Informationen zur Stammzellspende zum Download.
Bei einer Knochenmarkentnahme wird dir unter Vollnarkose ein Knochenmark-Blutgemisch aus dem Beckenkamm entnommen. Dieses Verfahren wird bei etwa 20 % aller Spenden angewendet.
Am Tag vor der Knochenmarkentnahme wirst Du in die Klinik aufgenommen. Dort finden ein Begrüßungsgespräch, eine körperliche Untersuchung und eine Blutabnahme statt. Am nächsten Morgen wird dann die Knochenmarkentnahme unter Vollnarkose durchgeführt.
Für die Spende wirst Du auf den Bauch gedreht und zwei Ärzte punktieren rechts und links deinen Beckenkamm mit einer stabilen Hohlnadel.

In der Regel genügen für die Entnahme zwei kleine Hautschnitte (ca. 0,5 cm), durch die der Beckenknochen mehrmals punktiert wird. Mit der Hohlnadel wird Dein Knochen punktiert, anschließend wird auf die Nadel eine Spritze aufgesetzt und das Knochenmark-Blutgemisch entnommen.
Die genaue Entnahmemenge wird durch die für den Patienten angeforderte Zellzahl bestimmt. Es gibt aber eine Obergrenze, die durch Dein Gewicht als Spender bestimmt wird. Grundsätzlich wird eine maximale Entnahmemenge von 1,5 Litern nicht überschritten. Das dabei entnommene Knochenmark entspricht etwa 5 % des Gesamtknochenmarkes.
Die entnommenen Zellen bilden sich innerhalb von zwei bis vier Wochen wieder nach.
Nach etwa einer Stunde wirst Du ins Aufwachzimmer gebracht. Dort liegst Du auf dem Rücken – um zu gewährleisten, dass die Punktionsstellen weiterhin gut abgedrückt werden, wird jeweils ein Sandsäckchen unter die punktierten Stellen geschoben.
Im Laufe des Tages darfst Du dann aufstehen, allerdings musst Du zur Beobachtung anschließend eine weitere Nacht in der Klinik bleiben. Insgesamt bist Du also rund 48 Stunden in der Klinik.
Nach der Entnahme kann es zu Beschwerden an den Entnahmestellen kommen, die oftmals mit einem Muskelkater oder einer Prellung im unteren Rückenbereich verglichen werden. Diese können bis zu 7 Tage anhalten und sehr gut mit einem Schmerzmittel (z.B. Paracetamol) behandelt werden.
Hier findest Du alle relevanten Informationen zur Knochenmarkentnahme zum Download.
Manchmal kommt es bei Patienten nach einer erfolgten Stammzelltransplantation zu frühzeitigen Rückfällen. Für diese Patienten ist oft die Gabe von Spenderlymphozyten erforderlich. Lymphozyten sind „aggressivere“ Zellen, die die Aufgabe haben, Krebszellen zu vernichten und das Immunsystem des Patienten zu stärken.
Die Entnahme von Spenderlymphozyten verläuft wie eine periphere Stammzellspende, allerdings ohne vorheriges Spritzen von G-CSF. Deine Spende wird ebenfalls mit einer Apheresemaschine durchgeführt, die das Blut durch Zentrifugalkraft in die einzelnen Bestandteile auftrennt und so das Sammeln der entsprechenden Zellen aus dem Blut ermöglicht. Dafür wird Dir an beiden Armen ein venöser Zugang gelegt, der über ein steriles Einmal-System mit der Apheresemaschine verbunden ist.

Dein Blut verlässt dann auf der einen Seite den Körper, fließt durch den Zellseparator und wird Deinem Körper auf der anderen Seite über den zweiten Zugang wieder zugeführt.
Die Spenderlymphozyten werden meist eingefroren (kryokonserviert) und später dem Patienten verabreicht.
Hier findest Du alle relevanten Informationen zur unstimulierten Leukapherese zum Download.
Die Suche nach einem passenden Stammzellspender für einen an Leukämie erkrankten Menschen beginnt im engsten Familienkreis. Die für eine Spende relevanten Gewebemerkmale (HLA-Merkmale) werden je zur Hälfte durch die Elternteile bestimmt. Dadurch liegt die Wahrscheinlichkeit bei 25 %, dass z.B. Geschwister die identischen Merkmale aufweisen und daher als Spender in Frage kommen. Mit neueren Therapieverfahren ist es auch möglich, dass nur zur Hälfte passende Familienmitglieder, sogenannte haploidentische Familienmitglieder, mögliche Spender sein können.
Für Fragen jeglicher Art haben wir immer ein offenes Ohr und unser Notfalltelefon ist rund um die Uhr erreichbar (+49 162 7162560).
Eine Spende für einen Familienangehörigen unterscheidet sich von einer Spende für einen Fremden. Als Angehöriger stehst du dem Patienten nahe und hast wahrscheinlich seine Leidensgeschichte miterlebt. In einer solchen Situation ist man natürlich in der Regel froh, helfen zu können. Allerdings ist oft auch der empfundene Druck höher und es können Sorgen und Anspannungen entstehen, z.B. weil man fürchtet, die eigene Spende könne das Familienmitglied vielleicht nicht heilen.
Sollte innerhalb der Familie kein passender Spender zur Verfügung stehen, kann in 80 % der Fälle in nationalen und internationalen Spenderdatenbanken auch ein passender Fremdspender gefunden werden.
Das medizinische Team der Cellex weiß um die besondere Situation, in der Du Dich als Familienspender befindest. Und genau aus diesem Grund wollen wir Deine Spende so angenehm und unkompliziert wie möglich gestalten.
Wir kümmern uns um alle organisatorischen und terminlichen Belange. Damit Du Dich ganz auf deine Spende konzentrieren kannst.
Spender FAQs
Wir von Cellex verstehen, dass Du bei einem solchen Thema noch viele Fragen hast. Die häufigsten Fragen haben wir hier gut auffindbar und übersichtlich aufgelistet für Dich dargestellt.
Häufig gestellte Fragen
Wie hoch ist die Wahrscheinlichkeit, dass ich als Spender in Frage komme?
Die Wahrscheinlichkeit, dass bei Dir eine Bestätigungstypisierung durchgeführt wird, liegt ungefähr bei 1:3. Hier wird noch einmal ganz genau überprüft, ob Du wirklich ein passender Spender bist und ob aus medizinischer Sicht nichts gegen eine Spende spricht. Nur einer von hundert registrierten Spendern wird später um eine Spende gebeten.
Wie hoch ist die Wahrscheinlichkeit, dass „mein Patient“ durch die Spende geheilt wird?
Der Erfolg der Stammzellspende hängt stark vom Gesundheitszustand des Patienten ab. Die Heilungschancen liegen durchschnittlich bei 40 bis 70%.
Bin ich der einzige Mensch, der für die Spende infrage kommt?
Prinzipiell ist es möglich, dass mehrere Menschen auf der Welt aufgrund ihrer genetischen Merkmale als Spender infrage kommen. Außerhalb der Familie des Patienten einen passenden Spender zu finden ist allerdings sehr viel schwieriger. Laut allgemeiner Einschätzung liegt diese Wahrscheinlichkeit zwischen 1:20.000 und eins zu mehreren Millionen. Jeder siebte Patient findet gar keinen passenden Spender.
Kann ich aussuchen, welche Entnahmemethode angewandt wird?
Grundsätzlich kannst Du Dich für eine der beiden Entnahmearten entscheiden, und wir versuchen natürlich, Deinen Wunsch nach einer bevorzugten Entnahmeart zu erfüllen. Es kann allerdings sein, dass Du als Spender nur für eine der Entnahmemethoden in Frage kommst. Welche Methode aus medizinischen Gründen bevorzugt oder sogar notwendig ist hängt von der Situation des Empfängers ab. Prinzipiell wäre es optimal, wenn Du zu beiden Entnahmearten bereit bist.
Kann ich meine zugesagte Spende zurückziehen?
Deine Spende ist grundsätzlich natürlich freiwillig und kann auch zurückgezogen werden. Entscheidest Du Dich jedoch kurzfristig gegen eine bereits zugesagte Spende, kann das fatale Folgen für den Empfänger haben, denn dieser wird vor der Transplantation intensiv auf Deine Spende vorbereitet. Sein erkranktes blutbildendes System wird mittels einer Chemo- oder Strahlentherapie „heruntergefahren“. Ohne den Erhalt Deiner Stammzellen hat der Patient oft keine Chance zu überleben. Wir bitten Dich daher, vor der Spendenzusage genau abzuwiegen, ob Du diese abgeben willst und kannst. Bei Fragen, Ängsten und Sorgen steht Dir das Cellex-Team rund um die Uhr zur Verfügung.
Was ist, wenn ich mir die GCS-F-Spritzen nicht selbst setzen kann/möchte?
Es ist nicht schlimm, wenn Du es nicht schaffen solltest, dir die vorbereitenden Spritzen selbst zu setzen. Du kannst einen Freund oder Bekannten darum bitten, das zu tun. Wenn auch das nicht möglich ist, dann werden wir dir einen Pflegedienst schicken. Dieser kommt zweimal täglich morgens und abends zu Dir nach Hause und setzt Dir die Spritze.
Wie ist der genaue Tagesablauf bei der Apherese?
Am Tag der Apherese triffst Du zwischen 7:30 und 8:00 Uhr in unserem Entnahmezentrum ein. Nach der Begrüßung wirst Du von dem zuständigen Pflegepersonal in den Apherese-Raum gerufen. Während der drei- bis fünfstündigen Entnahme kannst Du einen Film ansehen, Musik hören oder ein Buch lesen. Nur einer deiner Arme wird in der Bewegung eingeschränkt sein. Du kannst während der Entnahme auch auf die Toilette gehen. Am Ende der Entnahme kannst Du Deine Begleitperson telefonisch über die voraussichtliche Abholzeit informieren.
Nach der Spende solltest Du weitere 30 Minuten warten, damit wir Deine Fitness überprüfen und eventuell auftretende Fragen beantworten können. Während dieser Wartezeit erhältst Du einen elektronischen medizinischen Fragebogen, den Du ausfüllst und bei uns abgibst. Wir geben Dir auch die Broschüre mit Informationen über den Kontakt zwischen Spender und Empfänger. Am Nachmittag rufen wir Dich an und teilen Dir mit, ob am nächsten Tag eine zweite Spende erforderlich ist.
Werde ich Schmerzen bei oder nach der Spende haben?
Bei der peripheren Stammzellspende werden die Stammzellen aus der Blutbahn entnommen. Um die Anzahl der Stammzellen zu erhöhen musst Du Dir über vier Tage jeweils morgens und abends einen sogenannten Wachstumsfaktor unter die Haut spritzen. In dieser Zeit können als mögliche Nebenwirkungen grippeähnliche Symptome auftreten, vor allem Knochen- oder Gliederschmerzen. Diese können allerdings mit einem leichten Schmerzmittel (z.B. Paracetamol) behandelt werden.
Für die eigentliche Entnahme wirst Du an das Apheresegerät angeschlossen, indem Dir an beiden Armen ein venöser Zugang gelegt wird. Das Blut verlässt nun auf der einen Seite deinen Körper, fließt durch die Maschine und wird Deinem Körper auf der anderen Seite über den zweiten Zugang wieder zugeführt. Ein kleiner Teil des Blutes wird abgesammelt: die für den Empfänger wichtigen Stammzellen.
Damit das Blut im Verlauf des Verfahrens nicht gerinnt wird ein Gerinnungshemmer eingesetzt. Dieser Stoff kann kurzzeitig Symptome wie Kribbeln im Mund- und Lippenbereich oder in den Fingern verursachen. Diese Beschwerden können durch Kalziumgaben allerdings rasch behoben werden. Unserer Erfahrung nach wirst Du nach der Spende erschöpft sein, aber keine Schmerzen haben.
Bei der Knochenmarkentnahme werden Dir unter Vollnarkose Stammzellen aus dem Knochenmark entnommen. Für diese Entnahmeart ist keine Vorbereitung mit dem Wachstumsfaktor notwendig. Während der Entnahme spürst du keinerlei Schmerzen. Nach der Entnahme werden die Beschwerden an den Entnahmestellen oftmals mit einem Muskelkater oder einer Prellung im unteren Rückenbereich verglichen, die bis zu 7 Tage anhalten können. Du kannst bereits im Laufe des Entnahmetages wieder aufstehen.
Wie lange bin ich arbeitsunfähig?
Bei der peripheren Stammzellspende bist Du in der Regel nur an den Tagen der Entnahme arbeitsunfähig. Solltest Du allerdings wider Erwarten länger arbeitsunfähig sein, kann Dein Hausarzt Dir das bescheinigen.
Die Knochenmarkentnahme ist in der Regel mit einem 48-stündigen Klinikaufenthalt (inklusive Aufnahme- und Entlassungstag) verbunden. Die meisten Patienten sind nach der Knochenmarkentnahme 3 bis 5 Tage arbeitsunfähig.
Darf ich eine Begleitperson mitbringen?
Dies wird bei der ärztlichen Untersuchung besprochen.
Darf ich „meinen Patienten“ kennenlernen?
Bitte besprich diese Frage mit deiner Spenderdatei.
Wann erfahre ich, wie es „meinem Patienten“ geht?
Du musst Dich etwas gedulden, wenn Du erfahren willst, wie es Deinem Empfänger geht. Frühestens nach drei Monaten kannst Du bei der zuständigen Spenderdatei nach dem Gesundheitszustand Deines Patienten fragen. Bei manchen Kliniken und Ländern kann es etwas dauern, bis eine Antwort kommt, und in einigen Ländern ist jeglicher Kontakt zwischen Spender und Patient untersagt.
Glossar zum Freigabebrief
Sehr geehrte Spenderin, sehr geehrter Spender!
Anlässlich deiner Blutstammzell- oder Lymphozytenspende wird Dein Blut mehrfach untersucht. Im Freigabebrief zur Blutstammzellspende werden Dir Deine Ergebnisse mitgeteilt.
Der Freigabebrief wird von uns entweder direkt an Dich oder an die Datei gesendet. Solltest Du keinen Freigabebrief erhalten, wende Dich bitte an Deine Datei!
Wichtig für Dich: Sollte ein von uns erhobener Laborwert auffällig sein und eine unmittelbare medizinische Relevanz für Dich haben, wirst Du darüber umgehend informiert, bevor Du Deinen Freigabebrief erhältst.
Manche Laborwerte können von der Norm abweichen, ohne akut klärungsbedürftig zu sein. Sie können aber eventuell später eine Relevanz haben oder einfach nur kontrollbedürftig sein. Solche Abweichungen werden im Freigabebrief als Information für den Hausarzt erwähnt oder am Tag der Spende persönlich mit Dir besprochen.
Damit Du Deinen Freigabebrief besser verstehen und interpretieren kannst, haben wir für Dich dieses Glossar erstellt. Bitte beachte, dass manche Abweichungen von Normwerten ganz normal sind: 2,5% aller Laborwerte liegen immer ober- oder unterhalb dieser gezogenen Grenzen. Ob eine solche Abweichung von Relevanz ist oder nicht, ergibt sich dann erst in der Zusammenschau der Befunde.
albumen
Most of the protein in the blood is formed in the liver. Increases in the total protein content may indicate protein formation outside the liver. Decreases occur without clinical significance or indicate a deficiency in the state of loss. There are over 1,000 subforms of different protein molecules. Due to their physical properties, they can be separated in a so-called electrophoresis and divided into five main groups. The largest of these groups is albumin, a small molecule that takes over transport tasks in the blood. The result of electrophoresis is expressed as a percentage of the total protein. Changes should therefore always be considered relative to the other values.
albumin
See protein
basophils (leukocytes)
Basophils are a subgroup of white blood cells (leukocytes). Increases are most often found in donors with allergies.
beta HCG
Beta HCG is used to detect pregnancy. During and after menopause, the value is usually slightly higher.
bilirubin
Bilirubin is a degradation product of hemoglobin. This is divided into indirect bilirubin from erythrocytes and direct bilirubin from the liver and gallbladder. The most common is a slight (two- to threefold) increase in bilirubin in congenital metabolic variants (e.g. Meulengracht’s disease). These have no disease value. Caution is only advised when taking the painkiller paracetamol. If you have received paracetamol for a preliminary examination and Meulengracht’s disease has been diagnosed in the blood test, you will automatically receive an alternative, safe painkiller.
blood group and irregular antibodies
Each donor’s blood type is determined. It is divided into the blood groups A, B, AB, and O, and the rhesus subgroups c, C, D, e, and E. Blood group serological examinations primarily serve to inform the transplant center. For you as a donor, only the detection of irregular antibodies is relevant. If you should receive a blood transfusion at any time in your life, this information will help the blood bank to find the right blood for you.
blood sugar
Usually the blood sugar must be determined on an empty stomach. Since you usually have not fasted for the preliminary examination, the value is usually 1.5 to 2.5 times higher. That’s perfectly normal.
If the blood collection tube is not transported fast enough to the analysis laboratory, it may fall below the standard value. This shortfall is meaningless to you.
calcium
Calcium is an electrolyte of blood and the most important mineral component of bone. Changes occur with hormonal changes or disturbances of the bone metabolism. Calcium is also essential for the conduction and transmission of stimuli in the nervous system. With peripheral stem cell donation, your blood is led through a tube system into the cell separator. An anticoagulant must be used to prevent the blood from clotting during the collection procedure. We use an anticoagulant that is similar to citric acid and is quickly broken down by the body. This anticoagulant can cause a short-term calcium deficiency. A calcium deficiency manifests itself through symptoms such as tingling in the mouth and lip area or, for example, in the fingers. These complaints can be quickly remedied by calcium administration.
cholinesterase
Cholinesterase is an enzyme of the liver and enables statements to be made about liver function. Slight deviations from the standard value are of no relevance. A significant shortfall is found in a rare congenital form. In this case, a particular drug should not be administered during anesthesia for bone marrow collection.
coagulation diagnostics
Standard tests are performed to diagnose coagulation disorders (TPZ, Quick, PTT, INR). Slight changes are usually harmless and occur when the sampling tube has not been filled correctly or has been transported to the laboratory for a long time.
creatinine
Creatinine is a breakdown product from muscle metabolism. Creatinine is excreted completely through the kidney. Elevations can be seen in renal dysfunction. More often, our donors have an increase after sports or strength training.
CRP
The so-called C-reactive protein is a nonspecific inflammation marker. This value is increased in all forms of infections but also in smokers (due to chronic bronchitis). Slight elevations that can be explained by further findings (e.g. latent urinary tract infection) do not require further examination. If the increase is high, you will be contacted by our Cellex doctors. If necessary, the value must be checked again.
cytomegalovirus (CMV)
CMV is a herpesvirus and is usually transmitted as a droplet infection in young adults. The proportion of CMV positives (CMV IgG pos.) therefore rises with age to over 50% of the population. CMV can also be transmitted through blood and blood products. The detection of CMV IgM indicates a recent CMV infection. In this case, the blood sample is further analyzed (e.g. with direct detection of the virus DNA) to assess the risk of transmission for the recipient. If the risk of transmission is high, this can lead to a postponement of the donation. The level of these values is of no relevance to you. These values are only used to find out whether an infection occurred a short time ago or a long time ago.
Ebstein-Barr virus (EBV)
EBV is a herpesvirus that is most commonly transmitted in young adults via droplet infection (Pfeiffer’s disease). EBV can also be transmitted through blood and blood products. It is tested how long ago the EBV infection occurred and whether transmission to the recipient is likely. An acute or very recent EBV infection in the donor can lead to spleen enlargement. Since the stem-cell-stimulating drug also leads to spleen enlargement in the peripheral donation, in the case of an acute EBV infection, the peripheral donation must be postponed or a change to the bone marrow collection procedure must be made.
The infection parameters are specified as titer levels or units. The level of these values is of no relevance to you. These values are only used to find out whether an infection occurred a short time ago or a long time ago.
eosinophils (leukocytes)
Eosinophils are a subgroup of white blood cells (leukocytes). They serve as immunological defense against parasites and are involved in hypersensitivity reactions. Elevations are typically observed in donors with allergies. Reductions are generally of no relevance. In the case of peripheral stem cell donation, the ratio of leukocytes to each other (differential blood count) may also change four weeks after donation. However, this is of no relevance.
erythrocyte indices
Red cell indices include MCV, MCH, MCHC, and RDW. They provide information on the size and hemoglobin content of erythrocytes. Deviations can only be interpreted in the synopsis of all indices.
erythrocytes
Erythrocytes are the red blood cells. They contain the hemoglobin and transport oxygen from the lungs to the end organs. Changes in erythrocyte count can only be seen in the interaction of other values (hematocrit, MCV, MVH, and MCHC). The MCV (mean corpuscular volume) of erythrocytes is most frequently altered. MCV is typically reduced in iron deficiency, but increased in folic acid or vitamin B12 deficiency.
ferritin
Ferritin is a transport molecule for iron in the blood. Increases are often observed in infectious diseases and inflammations. Decreases indicate an iron deficiency. If the ferritin value has fallen below the lower standard limit, but the hemoglobin value is still normal, there is a latent iron deficiency. Even at this early stage, it makes sense to take iron as a medicine or dietary supplement.
gamma-GT (GGT)
Gamma-GT is an enzyme of the bile ducts and gallbladder. Slight elevations without clinical symptoms are usually irrelevant. Elevations can occur in liver disease and gallstones.
GFR
GFR (glomerular filtration rate) is a measure of renal function. The values are to be considered in connection with other kidney values, e.g. creatinine.
GOT (Syn. ASAT)
The GOT is an enzyme of the liver and erythrocytes. Elevations occur, for example, even with slight changes in the liver texture (e.g. fatty liver) but can also mean an increased decay of erythrocytes. Frequently the GOT is increased after a major sporting activity. The GOT must always be interpreted in a synopsis of further values.
GPT (Syn. ALAT)
GPT is an enzyme of the liver. Increases occur with changes in the liver texture (e.g. fatty liver). The GPT is more liver-specific than the GOT.
hematocrit
Hematocrit is the ratio of liquid blood components (plasma) to cellular components. The value is closely related to hemoglobin and is decreased in anemia.
hemoglobin
Hemoglobin is the red blood pigment and thus the transport carrier for the blood oxygen. Decreases occur in anemia. The most common form is iron deficiency anemia. Slight reductions (10–15% below normal) are not rare and often affect women (menstrual blood loss) or blood donors who regularly donate whole blood. Hemoglobin proliferation typically occurs during prolonged stays at high altitudes or among smokers.
With peripheral stem cell donation, you lose such a small amount of blood that it has no effect on hemoglobin levels. After bone marrow collection, the hemoglobin value may drop by one to three points. The initial value from the time before the donation is usually only reached again after three months.
hepatitis A (HAV)
HAV triggers infectious jaundice. It is transmitted via the fecal–oral route but can also be passed on via blood products. Most donors are already vaccinated against HAV or have the disease behind them. A current infection is detected by HAV-PCR.
hepatitis B (HBV)
HBV is transmitted through blood, blood products, and sexual contact. The acute infection can appear as jaundice and usually heals spontaneously. In some cases, it comes to a chronic course in which the affected persons are also contagious. Various test methods are used for the evaluation. The detection of so-called anti-HBs indicates immunity to HBV, usually by prior vaccination. The titer/unit height is irrelevant for you. Except in the case of occupationally exposed persons, it is not necessary to refresh the vaccination after successful basic immunization. Simultaneous detection of anti-HBs indicates a past (healed) HBV infection. If further virus detection is negative, these donors will be allowed to donate blood or stem cells.
The detection of HBsAG or HBV-PCR is an acute or chronic infection and donation is not possible.
hepatitis C (HCV)
HCV is transmitted through blood, blood products, and sexual contact. The detection of anti-HBC or HCV-PCR indicates contact with the virus. These persons are generally excluded from a donation.
In some cases, the anti-HCV test is erroneously positive. In this case, further investigations should be carried out. If the result cannot be confirmed and the HCV-PCR is negative, a release for donation can be made.
HIV-1/2
HIV is a retrovirus and triggers HIV infection. Anti-HIV-1/2 and PCR-HIV are tested. In case of a positive detection, no donor release can take place.
HTLV-1/2
HTLV is a retrovirus transmitted through blood and sexual contact. The occurrence of HTLV is limited to a few regions of the world (e.g. Japan). Infections therefore do not actually occur in Germany. Nevertheless, we are all obliged to test donors to that effect. False-positive tests occur and are then further tested in a reference laboratory. If these retests are negative, a donation may be made.
LDH
LDH is an enzyme that is present in all body cells. “Wrong” elevations are often due to improper blood collection (too-fast aspiration) or too-long transport of the tube to the laboratory. Real elevations are rare and indicate increased cell turnover. This occurs, for example, after banal colds but also in congenital or acquired forms of anemia.
leukocytes
Leukocytes are white blood cells. Leukocytes can be further divided into neutrophils, lymphocytes, monocytes, eosinophils, and basophils. An increase in the number of leukocytes is typically found as a reaction to infections but also under stress conditions, e.g. after bone marrow donation. A reduction in leukocytes occurs in the case of a cold or educational disorders. The differential blood count is always used to interpret the leukocyte values.
In preparation for the peripheral stem cell donation, donors receive the drug Granocyte, which stimulates the leukocytes in the bone marrow. The upper standard value can be exceeded several times (three to eight times). This increase in the number of leukocytes gradually decreases after the donation and the cells are broken down by the body. This can take up to three weeks. During the follow-up examination by the family doctor four weeks after donation, the leukocyte value is usually already normalized again. Often it is also slightly lower than the initial value. This has no relevance to you.
lymphocytes
Lymphocytes are a subgroup of leukocytes. Lymphocytes serve as a specific defense against infections. Minor increases or decreases occur in both acute and declining infections. In the peripheral stem cell donation, the lymphocytes with the leukocytes are increasingly released into the blood and slowly degraded again after the donation. Temporary deviations from the norm value are frequent four weeks after donation but are of no relevance.
In lymphocyte donation (DLI), these cells are specifically collected. Apheresis causes you to lose about 20 to 30% of the lymphocytes circulating in the blood. This has no effect on any susceptibility to infection. The initial values are usually reached again after a few days.
malaria
Malaria is a mosquito-borne disease that frequently occurs in countries close to the equator. A visit to one of these countries would lead to a four-month ban on donating blood. As a rule, transplant centers accept shorter periods for stem cell donors. In individual cases (e.g. stay in a high-risk area without malaria prophylaxis or fever attack during the stay), further tests for malaria diagnostics are carried out (e.g. malaria antibodies, malaria PCR, thick drops).
MCH
See erythrocyte indices.
MCHC
See erythrocyte indices.
MCV
See erythrocyte indices.
monocytes
Monocytes belong to the white blood cells (leukocytes). They serve the specific defense against infections. Slight changes in the differential blood count are usually without relevance.
neutrophils (leukocytes)
Neutrophils belong to the white blood cells (leukocytes) and are the first guard in the defense against invaders and bacteria. They decompose and release toxic substances for bacteria. Elevations occur in all types of inflammation and especially in bacterial infections. Smokers often have slightly elevated values due to chronic irritation of the bronchial system. Slightly lowered values are usually without relevance; strongly lowered values rarely occur after drug administration (e.g. Novalgin). In peripheral stem cell donation, donors receive the drug Granocyte, which stimulates the neutrophil leukocytes in the bone marrow.
parvovirus B19
Parvovirus B19 is the pathogen that causes rubella. Parvovirus B19 can lead to a loss of the graft in stem cell transplant recipients; therefore, the infectivity of the donor is tested prior to stem cell donation.
phosphatase
Phosphatase is an enzyme of the bone metabolism and the bile ducts. Slight elevations occur in diseases of the bile ducts. Metabolic diseases should be considered in conjunction with other values (such as calcium).
potassium
Potassium is an electrolyte that is primarily excreted via the kidneys. Increases in potassium therefore occur in kidney dysfunction, and decreases in increased excretion (e.g. diuretic drugs).
In peripheral stem cell donation, potassium loss occurs due to the addition of citrate (citric acid) as an anticoagulant. You will therefore receive potassium-containing effervescent tablets or powder after the donation.
Often the potassium level is erroneously increased during laboratory tests if the sample has been transported over a longer distance (e.g. by post from the family doctor to the laboratory). As a result, the erythrocytes disintegrate into the sample tubes and release potassium.
sodium
Sodium is an electrolyte of the blood. Changes are rare and occur with hormonal disorders or rarely with severe fluid deficiency.
thrombocytes
Thrombocytes are the blood platelets that are responsible for blood clotting. Increased values are often found in infections or chronic inflammations. However, infections can also lead to a reduction in blood platelets. Rarely there is also an immunological degradation of the thrombocytes.
Since peripheral stem cell apheresis involves the collection of part of the blood platelets for technical reasons, the thrombocytes should not be less than 120 g/l on the day of the preliminary examination and donation.
After peripheral stem cell donation, the number of thrombocytes can be about one-third lower than the initial value; blood clotting is not affected. About one week after the donation, the thrombocyte values return to their original values.
thyroid diagnostics
If the TSH value is changed or if abnormalities are found in the thyroid ultrasound, further thyroid parameters are determined. These include the thyroid hormones fT3 and fT4 as well as antibodies against thyroid tissue such as MAK, TRAK, and TAK. The interpretation is done by our Cellex doctors, and relevant findings will be communicated to you immediately.
toxoplasmosis
Toxoplasmosis is an infectious disease caused by parasites transmitted by raw meat or cat droppings. The disease heals without consequences in people with a healthy immune system. About 50% of the population is infected (IgG positive). In the detection of IgM, the initial infection may have occurred only recently, which means that further investigations are necessary. A fresh or still-active disease with toxoplasmosis could trigger a disease in the recipient of the stem cell preparation, and the donation may have to be postponed until the acute infection has subsided.
TPPA (or TPHA)
TPPA is the detection of Treponema pallidum, the pathogen responsible for syphilis. In case of a positive detection, no donor release can take place.
TSH
TSH is a messenger substance that stimulates the thyroid gland to produce thyroid hormones. Changes can occur in both hyperfunction and hypofunction of the thyroid gland (see also “thyroid diagnostics”). If you are already taking a thyroid hormone supplement, the TSH level is usually normal or decreased. If there is an increase, the amount of thyroid hormone prescribed is too low.
urea
Urea is a degradation product of animal proteins. Increases are rather rare and must be interpreted with other kidney values.
uric acid
Uric acid is a degradation product of food containing purine (e.g. meat and fish) but also of the body’s own cells. An increase is not uncommon and can lead to a gout seizure with appropriate predisposition and dietary errors. In peripheral stem cell donation, drug stimulation increases the number of leukocytes three to eight times above the norm. These cells must then be broken down again by the body. This produces uric acid. The pre-examining Cellex physicians decide individually whether you will receive a preventive medication (allopurinol) to lower the uric acid level in order to prevent a gout attack.
urine status
The urine status with the help of a test strip (quick test) gives an initial overview of the function of the kidney and the urinary tract. Protein may be elevated after physical exercise or in urinary tract infections. The strongest indication for a bacterial urinary tract infection is the detection of nitrite (degradation product of bacteria) and leukocytes. The detection of erythrocytes is very common in women because the detection method is very sensitive and therefore positive results occur long after visible menstruation has stopped. In men, the positive detection of erythrocytes is most often due to a disturbance of the test strip by food components. If the results are unclear, we will arrange for the test to be repeated by the family doctor or the donor.
In the urine sediment, solid and cellular components of urine are evaluated under the microscope. This information is used to interpret the urine status. For example, the detection of squamous epithelia (cells from the urethra) indicates faulty sample collection (mid-stream urine).
varicella antibodies (VZV)
Varicella zoster is a herpesvirus and the causative agent of chicken pox. Some transplant centers require the detection of VZV before transplantation. The evidence is irrelevant to you.
WNV
West Nile virus is a disease transmissible by migratory birds that occurs in some countries of Eastern Europe and North America. Donors who were in these countries within four weeks before the donation in the period from June 1 to November 30 will be tested for this pathogen.